
Screening
Configure ALEA’s Screening and Enrollment Application to suit your trial. Generate screening numbers or have site staff enter their own. The ALEA Screening and Enrollment Application is complete and ready to use. And, you can instantly add extra fields and edit checks based on your trials’s requirement.
Randomization
The randomization service includes flexible form definition, unlimited stratification factors, unlimited number of treatments, blocked randomization, minimization, unequal allocation schemes, multi step randomisations, a simulation service which produces a comprehensive validation report, and more. It allows for re-use of components at the level of questions, forms and complete studies.
Drug Supply Management
The Drugs Supply Management supports both simple and complex drug distributions schemes. It includes per site resupply trigger levels and sizes, per site initial shipment sizes, upload of concealment lists, generating concealments lists, predictive drug supply through pDSM algorithms with deltaS deltaT site accrual prediction.
Medical Coding
For medical coding, ALEA is integrated with MedDRA and WHO Drug, enabling consistent classification, improved analysis, and efficient clinical reporting.
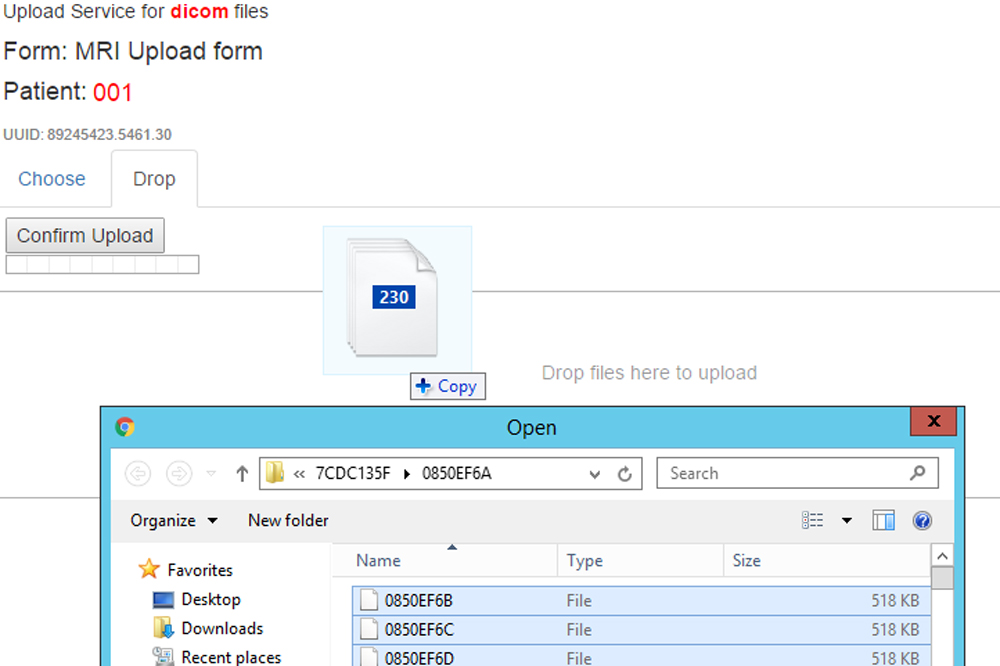
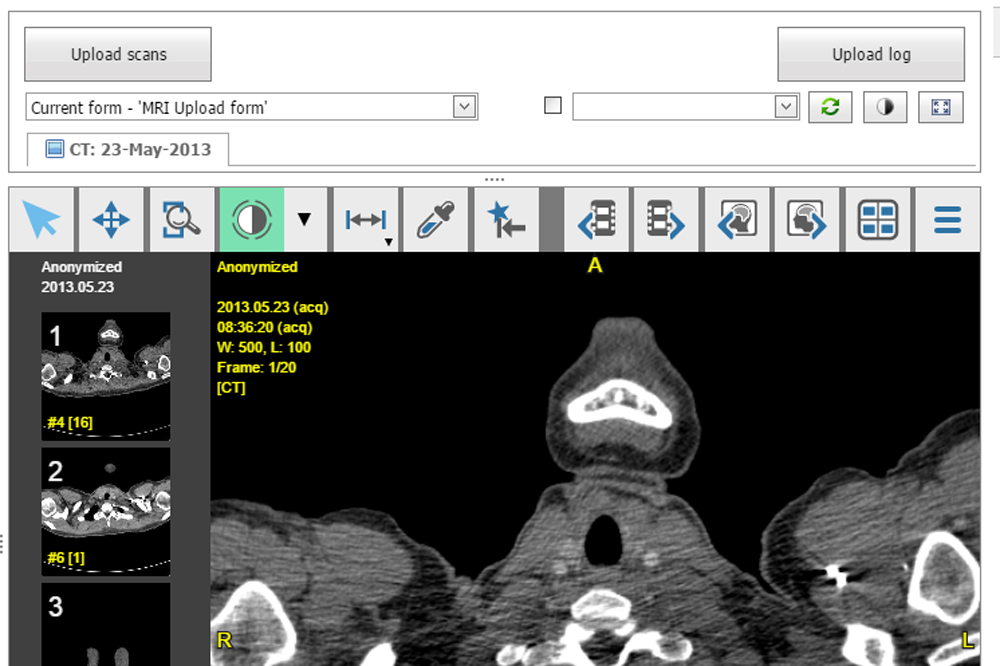
Imaging
ALEA supports multiple forms of imaging. including DICOM, video, image, PDF, FCS, and pathology attachments for centralized, efficient data management and analysis.
LAB
The LAB module facilitates lab normal values, enabling standardized ranges, consistent interpretation, and efficient analysis across studies and sites.
For more information regarding our product:
Electronic Data Capture
ALEA randomisation methods
ALEA randomisation supports the following methods of randomisation for healthcare trials. It supports trials with any number of treatment groups, and randomisation ratios other than 1:1.

Minimisation
The randomised groups are balanced on the basics of the characteristics of each participant. Each new participant is allocated to the group that has the fewest number of people like him or her at that time. The default setting is that the allocation uses simple randomisation only if there is no difference between the groups when the new participant is entered into the trial.
Minimisation may be configured in accordance with the options set out in Pocock and Simon’s paper. These settings determine how much the system biases the random allocation in favor of the underrepresented treatment group passes some threshold. This method can be used to help ensure balanced the patient characteristics within each group.
Block randomisation
Participants are allocated to the treatment group that is next in a block of allocations. Within each block, each treatment group occurs the same number of times. The user selects the block size for their trial as a whole or for specific parts of their trial.
Random block randomisation
To make it less likely that the next allocation can be predicted, this method varies the size of each block. ALEA Clinical chooses the size of each block by multiplying the number of treatments groups by a whole number between 1 and a minimum block size, set by the user.
Simple randomisation
Each participant has an equal chance of being allocated to any of the treatment groups, regardless of any imbalances that have already built up within the trial.
* Blinding
If participants in the trial are not to know which treatment they will receive, ALEA Randomisation can convert the treatment allocated into a box number or code, and returns this rather than the treatment. ALEA Randomisation helps the user to prepare these numbers or codes, so that the trial material can be prepared in advance.